People who consume psilocybin-containing mushrooms — otherwise known as magic mushrooms — typically undergo a surreal experience in which their sense of space, time and self is distorted. Advocates have long argued that, under the right conditions, psychedelic experiences can alleviate mental distress, and a smattering of scientific studies suggests they may be right. Understanding precisely how the drug affects the brain will help scientists and doctors harness its therapeutic potential.
In a new study, researchers at Washington University School of Medicine in St. Louis report that psilocybin, the active compound in magic mushrooms, temporarily scrambles a critical network of brain areas involved in introspective thinking such as daydreaming and remembering. The findings provide a neurobiological explanation for the drug’s mind-bending effects and lay some of the groundwork for the development of psilocybin-based therapies for mental illnesses such as depression and post-traumatic stress disorder.
“There’s a massive effect initially, and when it’s gone, a pinpoint effect remains,” said co-senior author Nico U. F. Dosenbach, MD, PhD, a professor of neurology. “That’s exactly what you’d want to see for a potential medicine. You wouldn’t want people’s brain networks to be obliterated for days, but you also wouldn’t want everything to snap back to the way it was immediately. You want an effect that lasts long enough to make a difference.”
The study, available July 17 in Nature, creates a road map other scientists can follow to evaluate the effects of psychoactive drugs on brain function, potentially accelerating drug development efforts for any number of psychiatric illnesses.
Psilocybin showed promise as a treatment for depression in the 1950s and ‘60s, but restrictive federal drug policy in subsequent decades quashed nearly all further research. In recent years, though, regulations have loosened, and interest in the field has been revived.
“These days, we know a lot about the psychological effects and the molecular/cellular effects of psilocybin,” said first author Joshua S. Siegel, MD, PhD, an instructor in psychiatry. “But we don’t know much about what happens at the level that connects the two — the level of functional brain networks.”
To fill that gap, Siegel pulled together a team including Dosenbach, who is an expert in brain imaging, and co-senior author Ginger E. Nicol, MD, an associate professor of psychiatry who has experience running clinical trials with controlled substances. Together, they devised a way to visualize the impact of psilocybin on individual participants’ functional brain networks – neural communication pathways that connect different brain regions – and to correlate changes in these networks with subjective experiences.
The team recruited seven healthy adults to take a high dose of psilocybin or methylphenidate, the generic form of Ritalin, under controlled conditions. Because psychedelic trips carry the risk of users having negative or scary experiences, a pair of trained experts stayed with each participant throughout the experience. The experts helped prepare the participants for what they were likely to experience, provided guidance and support during each experiment, and helped the volunteers process what had occurred afterward. Each participant underwent an average of 18 functional MRI brain scans in the days to weeks before, during and up to three weeks after their experiences with psilocybin. Four participants returned six months later to repeat the experiment.
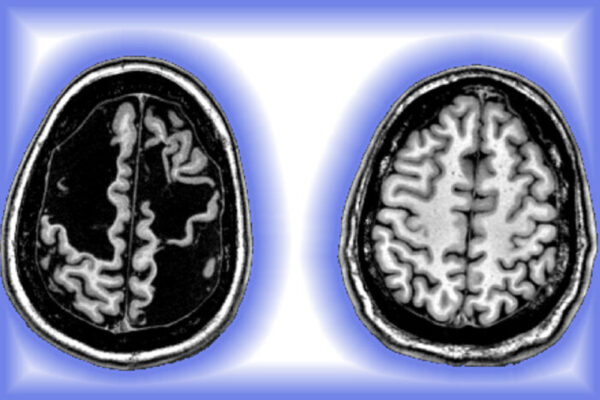
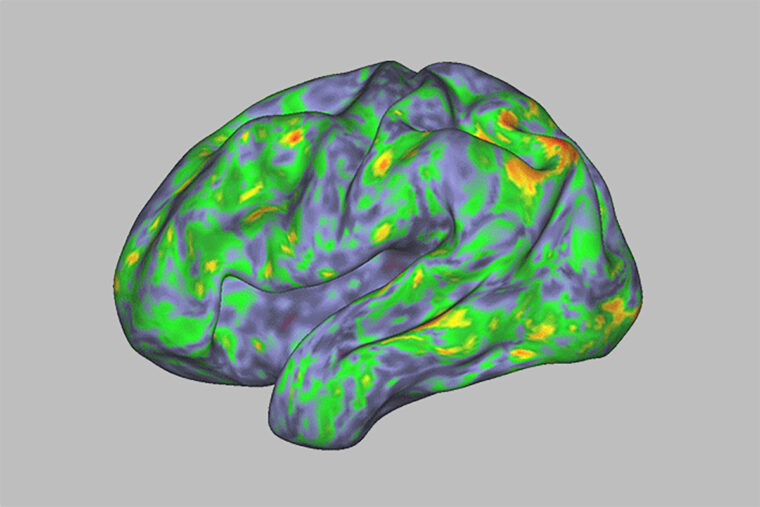
Psilocybin caused profound and widespread — yet not permanent — changes to the brain’s functional networks. In particular, it desynchronized the default mode network, an interconnected set of brain areas that, ordinarily, are simultaneously active when the brain is not working on anything in particular. After falling out of sync, the network re-established itself when the acute effects of the drug wore off, but small differences from pre-psilocybin scans persisted for weeks. The default mode network remained stable in people who received methylphenidate.
“The idea is that you’re taking this system that’s fundamental to the brain’s ability to think about the self in relation to the world, and you’re totally desynchronizing it temporarily,” Siegel said. “In the short term, this creates a psychedelic experience. The longer-term consequence is that it makes the brain more flexible and potentially more able to come into a healthier state.”
Normally, each individual’s functional brain network is as distinctive as a fingerprint. Psilocybin distorted brain networks so thoroughly that individuals could no longer be identified until the acute Effects wore off.
“The brains of people on psilocybin look more similar to each other than to their untripping selves,” Dosenbach said. “Their individuality is temporarily wiped out. This verifies, at a neuroscientific level, what people say about losing their sense of self during a trip.”
During the experience, participants were asked to rate their feelings of transcendence, connectedness and awe using the validated Mystical Experience Questionnaire. The magnitude of the changes to the functional networks tracked with the intensity of each participant’s subjective experience.
“We were able to get very precise data on the effects of the drug in each individual,” Nicol said. “This is a step toward precision clinical trials. In psychiatry, we often don’t know who should get a particular medicine and how much or how often. As a result, we end up prescribing one medicine after another, tinkering with the dosage, until we find something that works. By using this approach in clinical trials, we can identify the factors that determine who benefits and who doesn’t, and make better use of the medicines we have.”
Nicol, Siegel and Dosenbach emphasize that people should not interpret their study as a reason to self-medicate with psilocybin. The drug is not approved by the Food and Drug Administration (FDA) as a treatment for depression or any other condition, and there are risks to taking it without the supervision of trained mental health experts.
Siegel JS, Subramanian S, Perry D, Kay BP, Gordon EM, Laumann TO, Reneau TR, Metcalf NV, Chacko RV, Gratton C, Horan C, Krimmel SR, Shimony JS, Schweiger JA, Wong DF, Bender DA, Scheidter KM, Whiting FI, Padawer-Curry JA, Shinohara RT, Chen Y, Moser J, Yacoub E, Nelson SM, Vizioli L, Fair DA, Lenze EJ, Carhart-Harris R, Raison CL, Raichle ME, Snyder AZ, Nicol GE, Dosenbach NUF. Psilocybin desynchronizes the human brain. Nature. July 17, 2024. DOI: 10.1038/s41586-024-07624-5
This work was supported by the Taylor Family Institute Fund for Innovative Psychiatric Research; the Healthy Mind Lab; the McDonnell Center for Systems Neuroscience; the Washington University Institute of Clinical and Translational Science; the National Institutes of Health (NIH), grant numbers MH112473, T32 DA007261, NS123345, MH129616, MH121276, MH118370, NS124738, MH096773, MH122066, MH124567, NS129521 and NS088590; the National Spasmodic Dysphonia Association; the Ralph Metzner Professorship; the Tianqiao and Chrissy Chen Institute; Washington University’s Intellectual and Developmental Disabilities Research Center; the Kiwanis Foundation; the Washington University Hope Center for Neurological Disorders; and Mallinckrodt Institute of Radiology. Additionally, this study utilized data from the Adolescent Brain Cognitive Development study, supported by NIH grant U01DA041120.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health (NIH).
About Washington University School of Medicine
WashU Medicine is a global leader in academic medicine, including biomedical research, patient care and educational programs with 2,900 faculty. Its National Institutes of Health (NIH) research funding portfolio is the second largest among U.S. medical schools and has grown 56% in the last seven years. Together with institutional investment, WashU Medicine commits well over $1 billion annually to basic and clinical research innovation and training. Its faculty practice is consistently within the top five in the country, with more than 1,900 faculty physicians practicing at 130 locations and who are also the medical staffs of Barnes-Jewish and St. Louis Children’s hospitals of BJC HealthCare. WashU Medicine has a storied history in MD/PhD training, recently dedicated $100 million to scholarships and curriculum renewal for its medical students, and is home to top-notch training programs in every medical subspecialty as well as physical therapy, occupational therapy, and audiology and communications sciences.
Originally published on the School of Medicine website