The number of people evaluated for signs of stroke at U.S. hospitals has dropped by nearly 40% during the COVID-19 pandemic, according to a study led by researchers from Washington University School of Medicine in St. Louis who analyzed stroke evaluations at more than 800 hospitals across 49 states and the District of Columbia. The findings, published May 8 in The New England Journal of Medicine, are a troubling indication that many people who experience strokes may not be seeking potentially life-saving medical care.
“Our stroke team has maintained full capacity to provide emergency stroke treatment at all times, even during the height of the pandemic,” said lead author Akash Kansagra, MD, an assistant professor of radiology at Washington University’s Mallinckrodt Institute of Radiology (MIR). Kansagra sees stroke patients at Barnes-Jewish Hospital. “Nevertheless, we have seen a smaller number of stroke patients coming to the hospital and some patients arriving at the hospital after a considerable delay. It is absolutely heartbreaking to meet a patient who might have recovered from a stroke but, for whatever reason, waited too long to seek treatment.”
Nearly 800,000 people in the U.S. experience a stroke every year. It is the fifth leading cause of death and the leading cause of long-term disability. With advances in stroke care such as better diagnostic tools, surgeries to remove blood clots or repair broken blood vessels, and clot-busting drugs, people have a better chance of recovering from a stroke today than ever before – as long as they receive treatment promptly. Clot-busting drugs are generally safe only within 4½ hours of symptom onset, and surgeries are only possible within 24 hours of symptom onset. The earlier the treatment is started, the more successful it is likely to be.
Worried by the low numbers of stroke patients being evaluated at Barnes-Jewish Hospital and hearing similar reports from colleagues at other institutions, Kansagra – along with co-authors Manu Goyal, MD, a Washington University assistant professor of radiology and neurology, and statistician Scott Hamilton, PhD, and neurologist Gregory Albers, MD, both of Stanford University – set out to determine how pervasive the problem was.
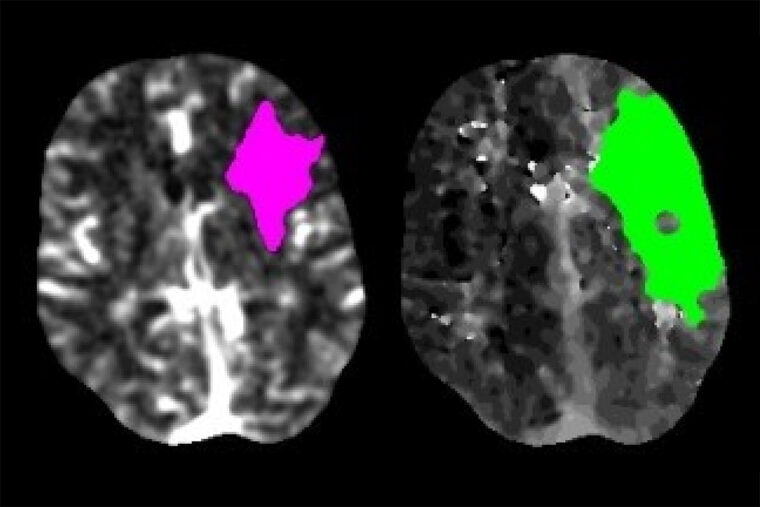
When patients arrive at a hospital and are showing signs of a stroke, they often get a brain scan so doctors can identify what kind of stroke has occurred and choose the most effective treatment. Many hospitals, including Barnes-Jewish Hospital, use software known as RAPID to analyze such brain scans. Kansagra and colleagues assessed how often the software was used in February, before the pandemic, and during a two-week period from March 26 to April 8, when much of the country was under shelter-in-place orders.
In total, the software was used for 231,753 patients at 856 hospitals representing the District of Columbia and all 50 states except New Hampshire. During February, the software was used for an average of 1.18 patients per day per hospital. During the pandemic period, software use per hospital averaged 0.72 patients per day, a drop of 39%.
“Across the board, everybody is affected by this decrease,” said Kansagra, who is also an assistant professor of neurosurgery and of neurology. “It is not limited to just hospitals in urban settings or rural communities, small hospitals or large hospitals. It is not just the old or the young or the people with minor strokes who aren’t showing up. Even patients with really severe strokes are seeking care at reduced rates. This is a widespread and very scary phenomenon.”
There’s no reason to believe people suddenly stopped having strokes. And the drop was large even in places where COVID-19 cases were few and hospitals were not overwhelmed, so patients should not have found it unusually difficult to obtain treatment.
“I suspect we are witnessing a combination of patients being reluctant to seek care out of fear that they might contract COVID-19, and the effects of social distancing,” Kansagra said. “The response of family and friends is really important when a loved one is experiencing stroke symptoms. Oftentimes, the patients themselves are not in a position to call 911, but family and friends recognize the stroke symptoms and make the call. In an era when we are all isolating at home, it may be that patients who have strokes aren’t discovered quickly enough.”
Common signs of a stroke include the sudden onset of numbness or weakness in the face, arm or leg, especially on one side of the body; speech difficulty; confusion; difficulty seeing or walking; and severe headache.
Even during a pandemic, it is critically important for people who may be experiencing a stroke to receive care immediately, Kansagra said. The risk of delaying care for a stroke is much greater than the risk of contracting COVID-19.
“The effect of coming in too late is the same in many respects as not coming in at all,” Kansagra said. “When patients come in too late, they may no longer be candidates for treatments that they would have qualified for just hours before. And as a result, they may not have access to treatments that are extremely effective in reducing death and disability.”
Kansagra AP, Goyal MS, Hamilton S, Albers GW. Collateral Effect of Covid-19 on Stroke Evaluation in the United States. The New England Journal of Medicine. May 8, 2020. DOI: 10.1056/NEJMc2014816
This is an unfunded investigator-initiated study.
Washington University School of Medicine’s 1,500 faculty physicians also are the medical staff of Barnes-Jewish and St. Louis Children’s hospitals. The School of Medicine is a leader in medical research, teaching and patient care, ranking among the top 10 medical schools in the nation by U.S. News & World Report. Through its affiliations with Barnes-Jewish and St. Louis Children’s hospitals, the School of Medicine is linked to BJC HealthCare.
Originally published by the School of Medicine
WashU Response to COVID-19
Visit coronavirus.wustl.edu for the latest information about WashU updates and policies. See all stories related to COVID-19.


