People with severe, treatment-resistant depression who received a nerve-stimulating therapy showed significant improvement in depressive symptoms, quality of life and ability to complete everyday tasks after a year, according to the results of a national, multicenter clinical trial led by Washington University School of Medicine in St. Louis. The findings are published Dec. 18 in a pair of papers in the journal Brain Stimulation.
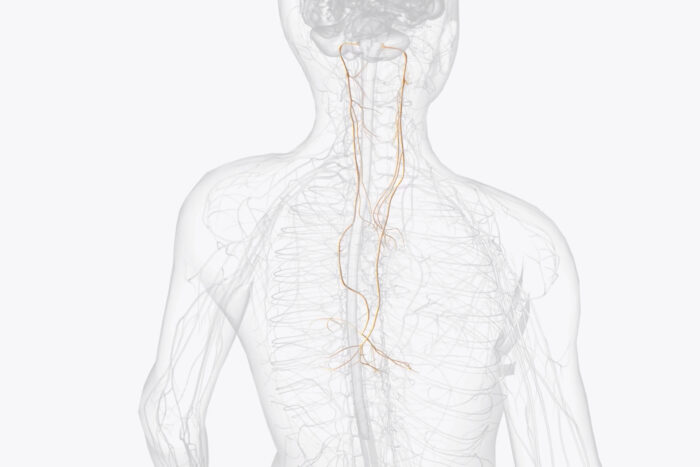
The study involved nearly 500 participants at 84 sites across the U.S. All of the participants suffered from severe depression that could not be treated effectively with medication or other approaches. This study represents one arm of the RECOVER trial; the other arm addresses bipolar depression and is ongoing. Three quarters of the participants were so ill they were unable to work. Each participant was implanted with a device that stimulates the left vagus nerve — a major conduit between the brain and the internal organs — but only half the devices were turned on. The researchers tracked the participants’ responses using multiple validated assessment tools. While the primary assessment tool revealed no significant differences between the on and off groups, many of the other measures showed significant benefits to using the device.
“These patients are extremely ill, and most have been for a very long time,” said Charles R. Conway, MD, a professor of psychiatry at WashU Medicine and the principal investigator of the RECOVER trial. “On average, each patient had already tried 13 treatments that failed to help them before they enrolled in the trial, and they had spent more than half of their lives sick with depression. But despite that super-high level of sustained illness, we still see statistically significant, measurable improvements in depressive symptoms, quality of life and functional outcomes.”
The improvements observed are potentially life-changing for these patients with severe, refractory depression, Conway said. Severe depression can render people “paralyzed by life,” unable to accomplish the tasks of daily living. The amount of improvement experienced by the participants could be the difference between being unable to get out of bed and being productive and effectively interacting with loved ones, Conway said.
A vagus nerve stimulation device was approved by the Food and Drug Administration (FDA) nearly two decades ago for treatment-resistant depression, but it has not become widely available. Between the cost of the device itself and the surgery to implant it, the therapy can be unaffordable for many patients, as the Centers for Medicare and Medicaid Services (CMS) and most private insurance plans currently don’t cover it.
Designed with an eye toward gathering the data that CMS needs to determine whether to cover the therapy, the RECOVER study aims to evaluate the effectiveness of vagus nerve stimulation therapy for treatment-resistant depression, both alone and as part of bipolar disorder. Many private health insurance companies follow the lead of CMS when it comes to coverage, so a decision by CMS to cover the device and the implantation surgery could make the therapy available to many more people. CMS helped design the RECOVER study and provided some funding.
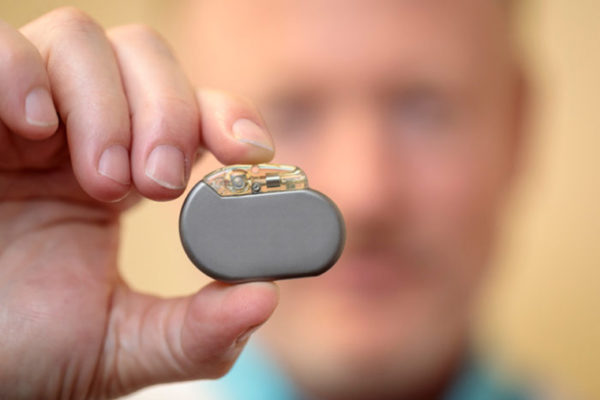
Vagus nerve stimulation therapy for treatment-resistant depression involves implanting a pacemaker-like device under the skin in the chest with a wire connected to the left vagus nerve in the neck. The device is part of the VNS Therapy System manufactured by LivaNova USA, Inc., which also sponsored and funded the trial in partnership with CMS.
The VNS Therapy device emits stimulation to the nerve, which in turn sends electrical pulses to areas of the brain associated with mood regulation. In this study, 493 people were implanted with devices and approximately half (249) of the devices were activated for the 12-month randomized control period. The other half of the devices did not have active stimulation during the control period.
The first two months of the 12-month trial period were dedicated to getting the devices’ electrical parameters properly adjusted to each patient. Starting in month three, the researchers obtained monthly evaluations of the participants’ depressive symptoms using four validated assessment tools, two of which were completed by blinded, off-site clinicians on the research team, one by an on-site psychiatrist or psychologist, and one by the patients themselves. The participants also rated their own quality of life and ability to perform the tasks of daily living every three months using three validated tools for quality of life and two for functional abilities.
All participants were already in treatment for depression and continued seeing their treating mental-health providers during the trial. Providers were discouraged from starting patients on new antidepressant treatments during the trial, but those who were already receiving treatments were encouraged to continue with them. Outcomes were measured in terms of the percentage of time participants experienced relief of depressive symptoms.
Overall, people with activated devices spent significantly more time with improved symptoms than did those with inactive devices. Complete remission was rare and did not differ between groups. People with activated devices also reported significant improvement in quality of life and functional abilities.
“What’s really important here is that patients themselves were reporting that their lives were improving,” Conway said. “You have a population of people that has been failed by a ridiculously high number of treatments, including very aggressive treatments such as electroconvulsive therapy. And they’re not just saying, ‘Yeah, I feel a little better.’ They’re saying they are seeing meaningful improvements in their ability to function and live their lives. And the nice thing about vagus nerve stimulation, we know from other studies, is that when the patient responds, the effects usually stick.”
Most of the improvements weren’t seen until the last three months of the trial. This finding was unsurprising, given that potential improvements from vagus nerve stimulation are known to progress slowly over the first year of treatment. At the end of the year, the devices that had been off during the 12-month control period were turned on. The primary outcome measure failed to show a significant difference between the two treatment groups, because the off group reported more improvement than expected, particularly in the last several weeks. Of note, all participants knew that the devices would be activated at year’s end, which may have affected those in the control group who knew potential relief was forthcoming, said Conway.
The participants will be followed for another four years to determine how long the effects last and how much the participants ultimately benefit. In addition, researchers are working on identifying patients’ characteristics tied to the greatest response.
Conway CR, Aaronson ST, Sackeim HA, George MS, Zajecka J, Bunker MT, Duffy W, Stedman M, Riva-Posse P, Allen RM, Quevedo J, Berger M, Alva G, Malik MA, Dunner DL, Cichowicz I, Banov M, Manu L, Nahas Z, Macaluso M, Mickey BJ, Sheline Y, Kriedt CL, Lee YC, Gordon C, Shy O, Tran Q, Yates L, Rush AJ. Vagus nerve stimulation in treatment-resistant depression: A one-year, randomized, sham-controlled trial. Brain Stimulation. Dec. 18, 2024. DOI: 10.1016/j.brs.2024.12.1191
Rush AJ, Conway CR, Aaronson ST, George MS, Riva-Posse P, Dunner DL, Zajecka J, Bunker MT, Quevedo J, Allen RM, Alva G, Luing H, Nahas Z, Manu L, Bennett JI, Mickey BJ, Becker J, Sheline Y, Cusin C, Murrough JW, Reeves K, Rosenquist PB, Lee YC, Majewski S, Way J, Olin B, Sackeim HA. Effects of vagus nerve stimulation on daily function and quality of life in markedly treatment-resistant major depression: Findings from a one-year, randomized, sham-controlled trial. Brain Stimulation. Dec. 18, 2024. DOI: 10.1016/j.brs.2024.12.1187
This study was organized and sponsored by LivaNova USA, Inc., the developer and manufacturer of the VNS Therapy System, and was designed and funded in partnership with the Centers for Medicare and Medicaid Services under its Coverage with Evidence Development program.
Conway has received research support from the American Foundation for Suicide Prevention, Assurex Health, August Busch IV Foundation, Barnes-Jewish Hospital Foundation, LivaNova, National Institute of Mental Health and the Taylor Family Institute for Innovative Psychiatric Research; consulted for LivaNova and Sage Therapeutics; and was a part-time employee at the John Cochran VA Medical Center in St Louis.
About Washington University School of Medicine
WashU Medicine is a global leader in academic medicine, including biomedical research, patient care and educational programs with 2,900 faculty. Its National Institutes of Health (NIH) research funding portfolio is the second largest among U.S. medical schools and has grown 56% in the last seven years. Together with institutional investment, WashU Medicine commits well over $1 billion annually to basic and clinical research innovation and training. Its faculty practice is consistently within the top five in the country, with more than 1,900 faculty physicians practicing at 130 locations and who are also the medical staffs of Barnes-Jewish and St. Louis Children’s hospitals of BJC HealthCare. WashU Medicine has a storied history in MD/PhD training, recently dedicated $100 million to scholarships and curriculum renewal for its medical students, and is home to top-notch training programs in every medical subspecialty as well as physical therapy, occupational therapy, and audiology and communications sciences.
Originally published on the WashU Medicine website